Case of the Month
Justine (not her real name), is a 31-year-old active lady who enjoys competitive netball. She presented to The London Foot and Ankle Centre in April 2018 with a history of three years of pain affecting both of her heels. Initially, her pain was only present first thing in the morning. She sought advice from podiatry and was recommended insoles, ice and massage. She had some physiotherapy and osteopathy as well. She also complained of some activity-related cramping in the front of her left leg. She does not have any problems with her Achilles tendon. She is generally very fit and healthy.
When she was examined, the area of tenderness was at the usual point where the plantar fascia attaches to the calcaneum (medial calcaneal tuberosity) with no real tenderness distally into the arch and no tenderness of her Achilles tendon or at its insertion. There were no signs that she was suffering from a tarsal tunnel syndrome or calcaneal stress fracture.
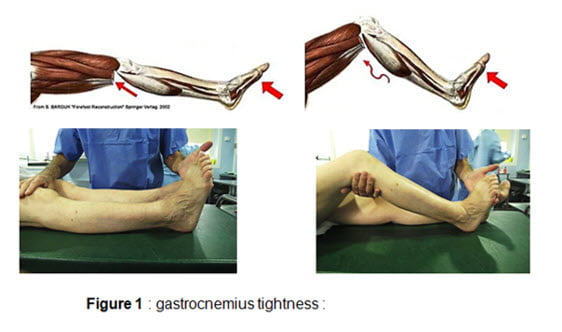
What was apparent, though, was that she has (naturally) very tight calf muscles. The Silfverskiold test showed that the tightness was limited to the gastrocnemius portion of the calf muscle (Figure 1). She had reduced forefoot ground clearance and great difficulty getting the ankle up to 90° when the knee was straight. With a bent knee, flexibility of the ankle was normal.
Imaging: An ultrasound scan confirmed thickening of the plantar fascia in both heels, to a maximum thickness of 5mm on the left side and 4.3mm on the right (normal is 3.5 – 4.0mm).
Treatment: Initially she was advised to try and stretch the calf muscles herself using exercises. It was explained that the tight calf muscle puts extra strain through the Achilles tendon and the plantar fascia. This inhibits natural recovery from plantar fasciitis. Approximately two months later she was reviewed and despite daily diligence with these stretching exercises she had only made a fraction of improvement.
She was offered further stretching exercises or surgical stretching of the tight calf muscle as an alternative. This is a day case operation under just local anaesthetic and sedation. She decided to try harder with her own stretches to avoid surgery, but by June 2018 she had come to realise that this was not going to be enough to help her.
Justine was admitted as a day case, and under light sedation with local anaesthetic (to the back of her knee), the medial head of the gastrocnemius muscle aponeurosis was stretched through a 2cm skin incision. She had to look after the stitches for two weeks but did not require crutches or a boot. She had some cramping symptoms initially, but when reviewed a few weeks later she was already 60% better.
At final follow up she described the surgery as amazing and life-changing and was back to playing netball.
At this last review, her only problem was the anterior muscle cramping symptoms (most likely a chronic compartment syndrome), and both she and I are hoping she will not require any surgical intervention for that.
Summary
This young lady is one of many patients who struggle to get rid of their plantar fasciitis symptoms simply because they have naturally tight calf muscles.
The tight calf muscle holds the foot in a slight tiptoe position, putting extra strain through the arch of the foot and the plantar fascia. This has a strong adverse effect on the ability of the body to naturally heal the plantar fasciitis. Several publications have shown how effective a small operation can be, if standard therapies fail.
If physiotherapy and home stretching exercises are not enough to improve the situation, there is an excellent chance that the very small surgical procedure will make the world of difference. This is a logical and effective way to treat stubborn case of plantar fasciitis. Trying to treat the pain with injections to the heel itself, or with shockwave therapy, when the gastrocnemius is tight is very rarely a good idea. This is because these “local treatments” to the heel are usually ineffective in the face of a tight muscle, since the resultant poor biomechanics increases the stress and strain in the foot.
References:
Gastrocnemius shortening and heel pain.
Solan MC, Carne A, Davies MS.
Foot Ankle Clin. 2014 Dec;19(4):719-38. doi: 10.1016/j.fcl.2014.08.010. Epub 2014 Oct 3. Review.
PMID:25456718
Proximal medial gastrocnemius release in the treatment of recalcitrant plantar fasciitis.
Abbassian A, Kohls-Gatzoulis J, Solan MC.
Foot Ankle Int. 2012 Jan;33(1):14-9. doi: 10.3113/FAI.2012.0014.
PMID:22381231
Surgical anatomy of the proximal release of the gastrocnemius: a cadaveric study.
Hamilton PD, Brown M, Ferguson N, Adebibe M, Maggs J, Solan M.
Foot Ankle Int. 2009 Dec;30(12):1202-6. doi: 10.3113/FAI.2009.1202.
PMID:20003880
Isolated gastrocnemius tightness.
DiGiovanni CW, Kuo R, Tejwani N, Price R, Hansen ST Jr, Cziernecki J, Sangeorzan BJ.
J Bone Joint Surg Am. 2002 Jun;84-A(6):962-70.
PMID:12063330


